

Teaching Manuals: A Resource for Body Mapping Educators
Section Four: Breathing
Why Musicians Need Body Mapping
-
Music serves and enriches our lives socially and personally.
-
Body Mapping makes it easier to create compelling and artistically satisfying musical performances.
-
Body Mapping has the potential to save musical careers.
-
Learning accurate information about the body in movement is the most efficient way to teach any musical skill.
-
Injury is at epidemic levels among student and professional musicians. This may lead to mental health issues that arise from being in chronic pain.
-
Body Mapping offers a framework for integrated movement to improve music making and alleviate pain and injury.
Moshe Feldenkrais - “When you know what you are doing, you can do what you want.”
Learning Objectives for Section Four
-
Breathing for music making can be free, coordinated and effortless.
-
Many misconceptions about breathing can be cleared up with Body Mapping.
-
Coordinated breathing will lead to improved whole body integration.
Learning Outcomes for Section Four
Teacher Goals
-
Clearly explains the structures and movement of breathing.
-
Effectively demonstrates and models simple movement exercises that help participants improve their breath awareness.
-
Appropriately summarizes how the structures of breathing are coordinate and how this coordination leads to integrated whole body awareness.
-
Explains how Body Mapping helps musicians find the appropriate sources of breath support for music making.
Participant Goals
-
Maps the structures and movements of breathing on self and is able to refine personal needs for remapping.
-
Accurately maps the pharyngeal space, including the tongue.
-
Understands structure, function and size of the diaphragm; specifically, identifying the location of the diaphragm and understanding its effect on rib movement and abdominal movement.
-
Understands structure, function and size of lungs.
-
Understands and experiences how inhalation and exhalation result from the dynamic volume/pressure relationship created by diaphragm, ribs and lungs working in coordination.
-
Learns how the balance of the arm structure can affect breathing, and how free breathing can permit greater movement freedom for musicians’ arms, hands and fingers.
-
Learns how a body in balance allows for the easy coordination of breathing structures, as well as the springy recoil of abdominal and pelvic muscles that support breathing.
-
Understands and experiences how spinal mobility contributes to the coordination of breathing movements.
Additional information can be found in the Section Four Supplement.
Please individualize your course regarding your own language, movement activities, and research.
Throughout the training manuals, text boxes highlight information that may be instrument specific, or may help clarify a concept. The trainee can decide when this information is appropriate for their audience.
“My idea is to advocate for first sticking with the indisputable, because mapping the indisputable makes such a huge difference in the quality of breathing when it is truly mapped:
-
The location of the lungs
-
The fact that ribs move, increasing thoracic volume
-
The fact that the diaphragm is active on inhalation, not exhalation
-
The fact that no air goes into the belly
Then I want to talk about the matter of support, its five sources:
-
The floor
-
The bony structure
-
The rebound back of the ab wall
-
The rebound of the pelvic floor
-
The lengthening of the spine
The reason I want to talk about support is because it is where the magic lies. Securely mapping the indisputable will give you efficient breathing. Secure support will make the magic that wins auditions and pleases audiences. This is an instance of ‘the truth shall make you free,’ and of the corrective power of a changed body map.”
-Barbara Conable

Image 4.1 : Places of Balance Skeleton
All of our breathing structures are located around our central skeletal core. Easy, efficient breathing begins with balance. Balance around our weight-bearing, weight-delivering spines and legs is the best postural condition for breathing.
Unfortunately, many people are taught that air works more like a liquid than a gas, and that it fills our bodies from the bottom and works its way up. Body Mapping Educators map the movements of breathing accurately--from top to bottom.
Questions for Review
-
How has your understanding of weight bearing/delivering and balance (dynamic neutral) affected your perception of breathing?
-
How has it affected your breathing during musical performance?
-
How is your whole body use right now?
-
Are you experiencing functional efficiency?

Image 4.2 : Location of The Lungs
The lungs fill much of the thoracic cavity, sharing space with the heart and the thoracic vertebrae. Air enters through our nasal and oral spaces by virtue of the muscular action of the intercostal muscles (between the ribs), and by the diaphragm, triggered by the brain, based on information from chemoreceptors in the blood vessels and brain, or, in the case of singers and wind players, by intention. The behavior of air itself is a factor, air moving, as it does, from areas of higher density to areas of lower density. From the nose or mouth, air passes within the pharyngeal space, into the trachea, bronchial tubes, and lungs. Air moves from the larger airway passages to the smaller ones, entering the lungs from the center out.
Questions for Review
-
What do you notice in your body about how you breathe in everyday life?
-
What do you notice in your body about how you breathe when playing your instrument?

Image 4.3a : A/O Joint, Hyoid Bone, Larynx and Trachea in Context

Image 4.3b : A/O Joint, Hyoid Bone, Larynx and Trachea in Context
In order for the freest breathing to occur, it is important to map the structures. In the case of the hyoid bone, larynx and trachea, they are suspended near the skull and spine. This is a good place to have everyone think about the balance of their atlanto/occipital joint and the freedom of the neck muscles.
To locate the larynx, place the fingers of one hand on your neck and swallow. You will feel the larynx move up and down.
See Breathing Supplement, Image 3A-B

Image 4.4 : Nasal Passages
Our breathing brings air into our body through our nasal passages or our mouth. Nasal passages are lined with sense receptors, so we may feel the movement of air within our nasal passages. This sensory information tells us a lot about the air: its quantity, quality and speed. This information can be useful for both instrumentalists and singers.
We must not limit ourselves by mapping the nasal area as merely facial. We need to “think nose” all the way back to the nasopharynx. It is of great benefit for singers and wind players to feel the passage of air. Musicians who stay awake to that have an added bit of information available.
Activity
-
Have participants inhale and exhale through nose and through mouth.
-
Have them inhale quickly. Have them inhale slowly.
-
What do you notice? What do you feel?
-
What is the quality of your whole body response to doing this?

Image 4.5 : Mouth
Our mouth is not a thing, but a space, and it must be mapped this way. The oral space includes the roof of the mouth above, the muscular floor of the mouth below, the muscular facial cheeks at the sides, and the tongue within. Movement must be mapped as movements of the structures that form the space, not as a function of the space itself.
Our mouths, like our noses, are rich with sensory information. Tactile receptors continually offer information about the location of our sensitive surfaces, defining our boundaries, in this case, the palate, tongue, cheeks, lips and gums. In addition, tactile receptors offer information about anything that touches the skin, in this case, air.
Our mouths are the beginning of our digestive systems. Because the mouth is a nutrient-receiving structure as well as an air-receiving structure, the more common use of sense receptors here is gaining information about the movement of food and drink, but these receptors need to be recruited for breathing as well. This area serves two major functions, nutrient gathering and air gathering. When it is at rest, it is in air gathering mode.
Questions for Review
-
How would you say this?
-
What are your words that you would use to best describe this illustration?
-
What mapping changes did you need to make to understand this?

Image 4.6 : Pharynx
We need to make a clear distinction between throat and neck. This is a very important distinction for wind players who often substitute neck tension for support.
Your neck is the large muscle group that moves your head. Your throat comprises the smaller structures interior to the neck that speak and sing and swallow. The pharynx is long from top to bottom, having three sections, the nasopharynx, behind the nasal passages, the oral pharynx, behind the mouth, and the laryngeal pharynx, behind the voice box.
The muscles of the neck are for moving the head and must otherwise be free. The pharyngeal muscles are for swallowing and must otherwise be free. There are two types of pharyngeal muscles: the constrictors and the longitudinal pharyngeal muscles. These muscles are connected by fascia to the base of the skull and therefore affect head balance. There are also muscle connections between the pharynx and the muscles of the hyoid bone which therefore also affect the use of the arm structure.
Here is a link to the kenhub anatomy website that gives a lot of detail on all of the pharyngeal muscles.
https://www.kenhub.com/en/library/anatomy/muscles-and-walls-of-the-pharynx
Questions for Review
-
How has this distinction between throat and neck affected your relationship with your instrument (voice)?
-
What mapping changes did you need to make?
Some Common Mismappings
-
Where the air goes
-
Mapping the belly as initiating breathing
-
Bottom to top event - Filling fantasy
-
Location of Trachea and Esophagus

Image 4.7 : Tongue
We need to accurately label the tip, the blade and the root of the tongue.
An adult’s tongue is secured at its base just above the larynx and hyoid bone. The back third of the tongue forms a portion of the front of the throat. This portion of the tongue is more vertical. It is essential to map the full depth of the tongue into the throat, the full width of the tongue, in the throat and in the mouth, and its full length, in order to ensure the tongue’s dexterity.
The function of the root of the tongue is to participate in swallowing. The blade and tip of the tongue are capable of very complex movements such as aiding singers with diction, and instrumentalists with articulation and timbre. The function of the root of the tongue is NOT for pitch, timbre, or articulation.
Most muscles in the body move bones, but the tongue moves itself. It is a composite muscle with a complex fiber structure, making it capable of very complex movements. The tongue contains many muscles, not separated, as muscles usually are, by connective tissue. A very precise map of the tongue may be developed over time by the use of kinesthetic and tactile receptors to feel its varied movement and its edges.
Singers and wind players need to become very skillful at using the tongue, and at using only those tongue muscles required for the specific task. The freedom of the tongue is dependent on freedom of the neck.
This can also be a place to mention that free neck muscles (and balance of the head) can sometimes depend on finding freedom in the tongue and pharyngeal muscles as well. Violinists, in particular, sometimes jam the violin in and up, chronically tightening all those inner muscles which makes real head balance impossible.
Questions for Review
-
What does this all mean for you personally?
-
What are your challenges and mis-mappings with this information?
-
How has your map of the structure, function and size of your tongue changed?
Activity
To sense the full size of the tongue, actively stretch the tongue out of the mouth, then let it slowly release back until it is fully relaxed in the mouth. This exercise should increase the kinesthetic awareness of the ROOT of the tongue in relation to the whole tongue. The root needs to be free in phonation, and brass and woodwind tonguing.
See Section Four Supplement Image 7

Image 4.8 : Tongue Muscles and Hyoid Bone
The function of the extrinsic tongue muscles is to alter the tongue’s position, moving it back and forth, up and down, or side to side. This graphic shows the extrinsic tongue muscles in relation to other structures and muscles in the oral cavity.
It appears complex, so let’s break it down:
-
“Glossa” is a Greek word for “tongue.” So all the muscles with “glossus” as the second part of their name
are tongue movers. The first part of the name signifies the origin of the muscle. Therefore the hyoglossus originates at the hyoid bone; the palatoglossus, the palate; the styloglossus, the styloid process; and the genioglossus originates at the chin (“geneion” is Greek for chin).
-
Many of the other muscles pictured here assist or respond to movements of the extrinsic tongue muscles. [The glossopharyngeus is actually part of the pharynx (superior pharyngeal constrictor muscle) and is another example of how interdependent all these muscles are.]
-
Note the central role of the hyoid bone. The hyoid bone is a hammock-like support for the tongue (located below the root of the tongue), so that at rest the tongue can nestle freely in between the lower teeth. The hyoid bone is also connected to the larynx below, and the epiglottis and pharynx behind.
-
Within the tongue are also four intrinsic muscles that alter the tongue’s overall shape, making possible speech (articulation), swallowing, and eating. Intrinsic muscles allow the tongue to shorten and lengthen, broaden and narrow, curl and uncurl.
To summarize, the tongue is not just one muscle, but a complex structure consisting of many closely related muscular strands. Intrinsic muscles change the shape of the tongue and are not attached to any bones. Extrinsic muscles change the position of the tongue, and are secured to bone.
Section 4 Supplement for more about the tongue in articulation, and the hyoid bone. Image 7.

Image 4.9 : Moving Jaw (Lower Jaw)
The lower jaw (mandible) is an appendage that hangs from our skull and is very mobile. For anyone that has had braces or orthodontic work done, the orthodontist will often refer to the upper jaw (maxilla). The maxilla is part of your skull and includes your upper teeth.
For purposes of your body map and finding ease and freedom of your breath, you want to map the mobility of your lower jaw or mandible. The mandible is the lower jaw bone, an appendage that articulates with the skull on either side at the temporomandibular joints. Permit the ease and freedom of your skull on top of your spine, and allow your lower jaw to move to take a breath.
People with two movable jaws in their body map attempt to open their mouths in both directions as if both mandible and maxilla were equally mobile. Their attempt to open in both directions unnecessarily involves the whole head and neck in what should be a simple, local movement.

Image 4.10 : Mandible from Front and Side

Image 4.11 : TMJ (Temporomandibular Joint)
The TMJs are the joints of the mandible (the jawbone) and the skull at the base of the temples: temporomandibular joints.
See Section 4 Supplement Image 11

Image 4.12 : Location of the TMJ
Our TMJs are just in front of our ears, not behind them, as some people think, nor at the forward protuberances which slide along the cheekbones, nor just behind the teeth, nor at the bumps near the bottom of the ear lobes. These common mismappings cause forced, tense, strange movements of the jaw plus pain and injury for some people. As soon as the structure is accurately mapped the movement becomes free and efficient.

Image 4.13a : Jaw Closed and Open
Image 4.13a is an image of the jaw (colloquially known as the lower jaw) from the side, but it is also an image of how the jaw just drops open when the jaw closing muscles are released. The two jaw closing muscles shown above are the temporalis and the masseter muscles. Gravity and the weight of the jaw give us all the mouth space we need for breathing.

Image 4.13b : Jaw Opening Muscles
Image 4.13b shows the digastric muscle (highlighted in blue). It is a small muscle located in the neck. The name comes from the fact that this muscle has two different muscle bellies (anterior belly and posterior belly) that are joined together by a tendon. The function is to open the jaw further than opening with just gravity and release of masseter and temporalis muscles (as shown in Image 4.13a). Because of its connection to the hyoid bone, overuse of the digastric muscle has a direct effect on vocal sound.
Questions for Review
-
What have you learned about the mapping of your jaw and the TMJs?
-
How does the ease and freedom of your jaw aid in the ease and freedom of your A/O joint?
-
How does freedom in your tongue aid in the freedom for the jaw and consequently your A/O joint?
Common Mismappings
-
Size and structure of Tongue
-
Location of TMJs
Activity
Spend some time palpating your jaw. Know that the size and shape of the jaw is individual to each person. Let gravity release the jaw by its own weight. Allow a long slow breath and feel where the air passes the back of the throat. Now deliberately open your mouth fully, allow another breath. Feel the air flow, noticing that the air flows through a smaller space.

Image 4.14 : Facial Muscles
Many people think of the face as skin stretched over bone, not realizing the many facial muscles available for expression, resonance, shaping of vowels and consonants and forming of the embouchure.
It is important to map these muscles accurately as to function, especially the fact that they have nothing to do with raising or lowering pitch in singing, nor with lifting the soft palate.
See Section 4 Supplement Image 14

Image 4.15 : Facial Muscles
We must map our lip moving muscles, which extend from cheek to cheek and from the base of the nose to the base of the gums as distinguished from “lipstick lips” which are merely the specialized skin cells exterior to a small portion of the movement lips.
Singers and wind players may want to go into more detail about the lip moving muscles. The key thing to remember is that these muscles move as part of an integrated, whole body dependent on free neck muscles and skull/spine balance.

Image 4.16 : Pharynx
The base of the tongue and the pharyngeal muscles shape the boundaries of the pharyngeal space, and it is part of the alimentary (food) canal between the mouth and the esophagus. It is necessary to map this space from the nasopharynx into the oropharynx and then into the laryngeal pharynx.
Questions for Review
-
What is the relationship between the root of your tongue and your pharyngeal muscles?
-
How much ease can you permit in your throat, tongue, and neck when breathing to play or sing?

Image 4.17 : Pharyngeal Muscles
Map the pharyngeal MUSCLES as part of the digestive system. Nature simply gets double duty from this SPACE as from the mouth, using it for both nutrients and air. The muscles of the pharynx are active with regard to food and drink; they swallow food and drink. Air does not need to be swallowed, and pharyngeal muscles are not active in bringing in air, unless their function is mismapped. Some people tighten pharyngeal muscles, resulting in audible inhaling because of the constriction in the pharyngeal space. When the muscles are mapped as digestive, and not respiratory, they no longer constrict on inhalation. We inhale quietly, and as quickly as we need to, thus one does not have to do anything to have an “open throat”.

Image 4.18 : Trachea and Esophagus
The trachea, often called the windpipe, lying just under the skin in the front of our lower neck, is merely a passage for air on inhalation. On exhalation, however, its specialized top portion, the larynx, which contains the vocal folds, interrupts air, if we choose, and sets the air vibrating, resulting in singing or speaking or any of the other sounds we are capable of making.
The esophagus, which lies behind the trachea is the muscular tube for the passage of food and drink to the stomach. Incorrectly mapping the trachea as behind the esophagus can result in effortful breathing.

Image 4.19 : Trachea, Lungs and Bronchi
Air moves through the trachea, which divides into two tubes to deliver air to both lungs.
The tubes, called bronchi, divide many times to distribute the air efficiently to the entire lung. The smaller divided tubes are called bronchioles and air passes through their tiny ducts into elastic air sacs (alveoli.)

Image 4.20a : Anterior View of Trachea, Lungs, Bronchi, Heart and Diaphragm
Image 4.20b : Posterior View Lung, Heart and Bronchi


Image 4.21 : Lungs from the Front, Back and Side
Use this illustration to help your audience fully map the location, structure and size of the lungs. Our lungs, plus our heart, occupy the thoracic cavity, the space above the diaphragm, which is roughly the upper third of the torso. We need utter clarity about the location of our lungs. At rest, the top of the lungs is above the collarbones, the bottom of the lungs is near the lower tip of the sternum (the breastbone). Any fantasy that lungs are below the thoracic cavity will result in effort and distortion in breathing.
Our lungs lie under our upper ribs in back, and our shoulder blades lie over these ribs, serving as lung shields.
This picture shows our lungs in the context of our torso. We must understand that air goes no lower in the torso than the lungs. Very important movements of breathing happen lower in the torso than the lungs, but these lower movements must not be confused with air or with the movement of air, which flows in and out of our lungs, and no lower.
The lungs are not muscles, but sacs of tissue. Breathing exercises will neither strengthen the lungs nor change the base volume of the lungs. Surrounding muscles, including the diaphragm, will move the ribs, which in turn will alter the volume of the lung tissue.
Questions
-
What mismappings did you have about your lungs?
-
Was there anything that surprised you about your lungs?
-
How has accurately mapping the location of the lungs affected your breathing?

Image 4.22 : Lungs in Cross Section

We have 24 ribs, 12 on each side, 20 meeting springy cartilage in front and all meeting the spine in back. This means that we breathe with a minimum 24 breathing joints in back (more if you think of the ribs as articulating at 3 points), a breathing joint being where each rib moves in relation to the spine as we inhale and exhale. This swinging up and out, down and in, accounts for what scientists call the excursion of the ribs.
Ribs move at joints, like all other bones, by the action of muscles, in this case, the muscles that lie between the ribs, called the intercostals. The amount of rib excursion correlates with volume of air moved.
The movement of all the ribs can be felt, monitored and controlled. When we need maximum capacity, only totally free-moving ribs will acquire it. On exhalation, the descent of the ribs can be controlled so they make a long, slow, even excursion across a long phrase.
Image 4.23 : Ribs, Back View “Our Breathing Joints”
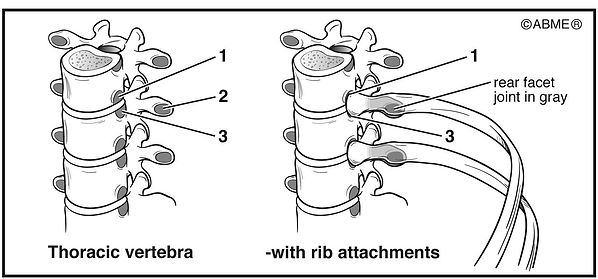
Image 4.23 (Continued) : Ribs, Back View “Our Breathing Joints”
The top rib and the bottom three ribs connect directly to their corresponding vertebrae. The rest of the ribs connect to two vertebrae, as shown in this inset. Numbers one and three show the approximate place where the head of a rib joins with two vertebrae. Number two shows the connection between the shaft of the rib and the transverse process of the lower of the two vertebrae. These joints are stabilized by ligaments. “Because of these many connections, movement of the ribs causes movement in the thoracic spine.” (Malde, WES, 4th edition, p 76)
This is an important learning moment for those musicians who have been trained to hold their ribs out, which includes many wind players and singers. If the ribs are not allowed their full excursion down and in on exhalation, there is no reflexive springing back up and out on inhalation.
See Section 4 Supplement Image 22 for more discussion of rib movement, including an activity.

Image 4.24a : Ribs, Front View

Image 4.24b : Ribs, Back View
We must forgo the use of the word ribcage. Cage is a terrible metaphor for ribs. The point of a cage is that the bars should not move. The point of ribs is movement. We don’t want our breathing to be caged; we want free breathing movements!
Also, a reminder: the shape of the ribs is more like that of a beehive than of a cage.
Breathing is movement. Rib movement is an important part of the whole movement of breathing. Ribs move at joints in back, but ribs move at cartilage in front. In the front, each of the ribs is attached to the sternum by an expanse of cartilage between the ribs and the sternum. Cartilage allows for rib movement because of its springy texture. Partly by virtue of the cartilage we deepen front to back as we inhale, and we widen side to side. Many muscles contribute to rib movements, but for breathing the primary muscles involved are the diaphragm and the internal and external intercostals.
Refer to Section 4 Supplement (Image 22 Ribs) for more information and activities about the ribs.
Activities
-
Our lower ribs (six on each side), except for our floating ribs, are attached to each other by cartilage. We may palpate the cartilage and feel its springy texture.
-
We may lay our hands along the cartilage and feel the movement of the springy cartilage in breathing.
-
We can also place hands under our armpits and feel the sides of the ribs.
Question
What do you notice about the shape of the individual ribs and the shape of the ribs together?

Image 4.25 : Diaphragm in Context of Whole Torso
At rest, the diaphragm domes high in our ribs. The diaphragm is a horizontal structure (not vertical) which divides the thoracic cavity above, from the abdominal and pelvic cavities below. Many people have mismapped the diaphragm as being located much lower than it actually is.

Image 4.26 : The Diaphragm is a Muscle
The diaphragm is a thin, dome-shaped layer of strong muscle fibers and connective tissue that spans the entire area between the thoracic cavity and the abdominal cavity. The base of the dome anchors along the lower ribs, including the lumbar spine and xiphoid process. The diaphragm’s descent (flattening somewhat) on inhalation aids the ribs in moving out and then up; its ascent (doming again) on exhalation is aided by the ribs coming down and in.
At rest, the diaphragm nestles inside the ribs slightly higher on the right side than the left. The diaphragm is anchored to the front of the lumbar spine by muscle fibers and tendons. At the top and center of the diaphragm, the muscle fibers radiate down and out from the central tendon. When the muscle fibers contract (on inhalation) the double dome shape of the diaphragm flattens somewhat. This downward movement of the central tendon pulls the heart and lungs downward, and helps swing the ribs up and out. These movements increase the volume of the chest cavity, causing air to flow into the lungs.

Image 4.27a : Diaphragm Viewed from Below Showing the Central Tendon

Image 4.27b : Diaphragm Viewed from Right Side Showing the Central Tendon and Heart
Ribs have their excursion in breathing, and the diaphragm has its excursion as well. The excursion of the diaphragm takes it from a highly domed position to a less domed position, thereby increasing the diameter of the thorax on inhalation. On exhalation, the diaphragm returns to its highly domed position in preparation for its next excursion downward and outward. Just as the ribs must make their full excursion down and in, so must the diaphragm make its full excursion back to fully domed if breathing is to be complete.
The movement of air in the lungs is related to Boyle’s Law*: When the thoracic cavity gets larger, the air pressure is higher outside than in the cavity and the resulting disparity in air pressure causes air to rush in and fill the lung tissue.
*Boyle’s Law: the pressure and volume of a gas have an inverse relationship, when temperature is held constant.
Here’s a brief video that clearly explains Boyle’s Law:
https://www.youtube.com/watch?v=q6-oyxnkZC0
The structures and movements described throughout this Section 4 Manual are mostly related to passive breathing. Breath coordination is similar whether one breathes passively or more actively. However, there will be more muscle groups involved in the active breathing that singers and wind players use to make music. More about this can be found in the Section 4 Supplement.
Questions
-
Any surprises about the location of your diaphragm?
-
What does the knowledge of the connection of the heart to the diaphragm via the central tendon mean to you?
Some Common Mismappings
-
Location and movement of Diaphragm
-
Rib Cage instead of individual Ribs
-
Column of Air Fantasy
-
Lungs push the ribs open
See Section 4 Supplement, Image 26 for information about other muscles that contribute to breathing
for singing and wind playing, as well as a description of a “box breathing” activity.

Image 4.28 : Excursion of the Diaphragm and Movement of the Pelvic Floor
The diaphragm’s movements on inhalation and exhalation affect structures below it. In the diaphragm, movement receptors are sparse compared to their density in the limbs and trunk, so we need to sense the diaphragm’s working by its effects in the movements of abdominal viscera (organs and gut) and the pelvic floor. This can be compared to sensing the working of the heart by feeling the pulse.
Video: 3D View of Diaphragm
https://www.youtube.com/watch?v=hp-gCvW8PRY
Video: MRI showing effects of diaphragm movement
https://www.youtube.com/watch?v=u-O8CgkCW1I

Image 4.29 : The Abdominal Wall
The abdominal wall is a layered cylinder of muscle surrounding our viscera in front, sides and back. On inhalation, the descending diaphragm puts pressure on this abdominal cylinder. The pressure put on the abdominal wall by the viscera being moved outward and downward by the descending diaphragm is equal in all directions. The viscera move outward against the entire cylinder, and the movement should be felt all around, not just in front. Recognize that the abdominal muscles do not initiate either inhalation or exhalation. Rather, they respond to, and coordinate with, the movements of the diaphragm and ribs on both inhalation and exhalation.
It is necessary to say something about appropriate effort. Abdominals actually do work during the movement of breathing, but in coordination with the whole body. Tone is a good word to describe what we want to feel in these muscles; tone being the dynamic character proper to the muscles of our bodies. If your muscles are properly toned they will do the work you need them to do, without the need for either overwork or underwork.
How do we know what the appropriate amount of effort is? This is the process that occurs in the practice of figuring out the amount of air for the phrase being played or sung and amount of effort needed to do it. It is a dynamic balance depending on the demands of the music.
See Section Four Supplement, Image 28 “The Abdominal Wall”
Question
How does breathing feel different for you when you allow movement of the entire abdominal cylinder, rather than just the front of the abdominal wall?

Image 4.30 : The Abdominal Muscles
Singers and wind players use the breathing apparatus energetically to create a tremendous variety of musical results. Abdominals can increase the speed, force and degree of exhalation by moving the organs upward against the diaphragm and pulling down and in on the lower ribs. These actions decrease thoracic volume, increasing pressure on the lungs to promote exhalation. Gentle engagement of the abdominal muscles allow singers and wind players to extend and enhance exhalation as needed. However the abdominal muscles do not necessarily have to contract during exhalation. Free and springy abdominal muscles support free, flexible music making.
Activity
Have students tense the abdominal muscles, and inhale, exhale, and then relax the abdominal muscles and inhale. Notice how much more easily the whole torso responds to inhalation, when the abdominals are relaxed. Excess tension in abdominal and pelvic floor muscles can invoke the valsalva maneuver, making breathing much more effortful.
What is Core Control/Stability?
Taken from PAMA Essentials of Performing Arts Medicine Course
-
We are not talking about abdominal strength: control is not strength.
-
The appropriate amount of stiffness/strength for the anticipated load. (Panjabi MM, 1992)
-
Balance of forces - “As much as necessary, as little as possible” Alan Lee
-
Dynamic control of the movement and the position of the trunk in relation to the pelvis and shoulder girdle. Kibler WB, Press J, Sciascia A (2006) The role of core stability in athletic function. Sports Medicine 36 (3): 189-198.
-
Proximal stability for distal mobility.
-
Core stability optimizes the production, transfer and control of movement and load during functional tasks (through the kinetic chain).
We are talking about a synergistic relationship between the transversus abdominus, lumbar multifidus, the pelvic floor and the diaphragm. These are the muscles that aid in the distribution of load throughout the skeletal, muscular and fascial systems. Remembering that in the physical therapy model, stability does not necessarily mean holding, it means that the muscles surrounding a structure (ie: shoulder blade or pelvis) are working together for ease of movement. Obviously, if you’ve had issues (previous surgeries, injuries, etc.) you may want to see a medical provider who has experience working with musicians.

Image 4.31 : Diaphragm, Posterior Abdominal Wall and Interior Muscles of the Pelvis.
We want to map the interior structures as we watch what changes occur with the exterior structures. This image puts into context the interconnectedness and the relationship between the diaphragm, psoas and pelvic floor muscles for free and easy breathing. As teachers we look for interruptions in a student’s overall balance throughout the body that may be interfering with this.
Refer to Section 4 Supplement Image 30 for information about the muscles of the “Abdominal and Pelvic Cavities” including the Psoas.

Image 4.32 : Pelvic Floor Muscles Viewed from Above
The pelvic floor is the muscle group that lies between the pubis and the sacrum front to back and between the sitting bones side to side. These muscles ideally should move responsively with the breath. Their movement should not feel like work.
If our pelvic floor muscles work (as in Kegel exercises, for instance) as we inhale, we compromise the excursion of the diaphragm; if our pelvic floor muscles work on exhalation we interfere with the springing back to neutral of the pelvic floor.
Some musicians are taught that tucking the pelvis, and/or tightening the glutes, provides extra support for breathing. Quite the opposite is true. When the pelvis is tilted forward or the glutes are tightened, then the resilience of the pelvic floor muscles will be inhibited. This tucked position also disturbs the overall alignment of the torso to the legs joints, obstructing one’s access to the support of the ground. The best support for breathing comes from good overall alignment, allowing muscles the freedom to be responsive to musical needs.
See Section 4 Supplement, Image 31 “Pelvic Floor Muscles”
Question
Can you permit the ease and freedom of your pelvic floor muscles while breathing?
Activities
-
Experiment with clenching the muscles of your pelvic floor and breathing, and then releasing and breathing. What are the differences in your experience?
-
Repeat the experience tightening your gluteal muscles and then your thigh muscles.
-
This can be done sitting or standing.
-
Squatting is a great way to feel the reflexive action of the pelvic floor. Experiment with squatting a little: (similar to Alexander Technique “monkey” position) and then more deeply, while noticing how this affects inhalation and exhalation. Then explore singing or playing an instrument in the squat position.

Image 4.33 : The Coordination of Movement of the Diaphragm and the Pelvic Floor Muscles
As the diaphragm descends it exerts pressure on all the viscera that lie between the diaphragm and the pelvic floor. The viscera are moved outward against the abdominal wall, and they are also moved downward against the pelvic floor where they do not meet the resistance they meet at the pelvic bones. Therefore, the pelvic floor descends as the diaphragm descends (unless it is tightening). When the diaphragm ascends the pelvic muscles ascend because the pressure from the viscera is taken off. This elastic recoil, or springing back of the abdominal wall and the pelvic floor is a dynamic, lively sensation, to be distinguished from the sensation of work in these areas. Voluntary work in these areas interferes with their natural involuntary action. Tone is a good word to describe what we want to feel in these muscles, tone being the dynamic character proper to the tissues of our bodies.

Image 4.34 : Spinal Mobility
From The Breathing Book by Amy Likar:
Spinal excursion is a powerful motion that coordinates the movements of breathing. It is an involuntary motion; we don’t do it, we allow it. If you allow spinal excursion as you play or sing, all of the movements of breathing can occur in coordination with one another.
As you inhale, your spine moves, gathering to accommodate the movement of your ribs, and your torso gets deeper and wider. As you exhale, your spine will lengthen, if you allow it, as your ribs glide back down and in. Another way of saying it would be your torso gets deeper and wider when you inhale and the mobility of the spine and ribs guides this deepening and widening. As you exhale, your ribs will move down and in and your spine will lengthen in response. This important motion of breathing, known as spinal excursion, will only happen if you have an overall whole body balance as you play including easy, mobile arms and legs.
Videos of Spinal Mobility in Breathing:
https://youtu.be/GG3xUGi9MGk & https://youtu.be/HrCEh90hbx0
See Section 4 Supplement, Image 33, “Spinal Mobility” for more information about gathering/lengthening, deepening/widening.

Image 4.35 : Coordination of Breathing Cycle
This illustrates the whole breathing cycle: inhalation on the left, exhalation on the right. Notice that the spine coordinates the movements of breathing. The gathering, deepening, and lengthening of the spine in breathing is involuntary. We do not need to do it; nature does it for us. We do, however, need to cooperate with it, and we certainly need not to interfere with it.
The spine’s mobility on inhalation facilitates the excursion of the ribs up and out and it facilitates the excursion of the diaphragm. The spine’s lengthening on exhalation facilitates the return movements of the ribs and diaphragm.
Breathing is like a Wave
When there is no unnecessary muscular holding, breathing movement occurs throughout the whole torso in an organized, wave-like pattern, top to bottom. As the lungs fill with air, the torso gathers slightly, the ribs move up and out, and the diaphragm descends, moving the contents of the abdominal and pelvic cavities outward against the abdominal wall (front, sides and back) and downward against the pelvic floor. As the lungs empty of their greatly-altered air, the torso lengthens slightly, the ribs move down and in, and the diaphragm ascends, allowing the contents of the abdominal and pelvic cavities and the pelvic floor to spring back.
Activities
-
Observe your breathing lying over a physioball. Experience how spinal mobility coordinates all the movements of inhalation and exhalation.
It is critical that students permit spinal excursion and not fabricate it. In standing, it is a more subtle sensation, it won’t be as drastic as when draping over a ball or a pillow. Those who try to feel the amount of movement standing that they see on someone else lying down will tend to fabricate the movement of gathering and lengthening while breathing. There is a difference between moving the spine and permitting spinal mobility while breathing. -
Ask your students to lie on the floor, knees bent, with their head barely touching a wall, using a thin book under their head to maintain head balance. Ask them to exhale fully so that they feel the top of their head nudging gently into the wall. Monitoring their rib movement with their hands, ask them to inhale deeply feeling the 360 degree expansion throughout the torso. While they keep their necks free, and eyes and noses pointing to the ceiling, ask them to notice how the top of their heads are now not in contact with the wall. As they exhale, they should notice how the head returns to its nestling against the wall. This is one way for students to experience the gathering and lengthening of the spine as it is coordinated with breathing.
Videos: Melissa Malde demonstrates how to increase awareness of spinal mobility using a physioball
https://vimeo.com/410256489/60de2d6e1a
Here is a link for David Nesmith’s “Breathing Hour Video Clips”, which can be purchased for use in the course: http://www.smartpoise.com/video/breathing-hour-video-clips/ The video includes five perspectives
demonstrating spinal mobility during free breathing. ”Each perspective is presented in real time (2 min clip) and enhanced 3x speed (1 min clip). The enhanced rate shows the breathing movement more dramatically, so when viewing the normal rate again, students usually see the wave-like motion more clearly.”

Image 4.36 : Head-Spine Relationship
Our heads are the context for our breathing structures because of the head’s relationship to the spine. In vertebrate movement, the head leads and the spine follows. Our neck must be free so that it does not interfere with the dynamic relationship of the head and the spine.

Image 4.37 : Releasing Into Length; Up and Over
Since the skull sits at the top of the spine, it can respond to the lengthening spine on exhalation, gently and subtly tipping up and over—IF your neck muscles are tension-free.
This slight moving away has been called “up and over” by vocalists; it was called “forward and up” by F.M. Alexander as he liberated it in his own reciting of Shakespeare.
Because the skull sits at the top of the spine, IF the neck muscles are chronically tight, the head will get pulled down, compressing the spine. The subtle tipping “up and over” will not be allowed in experience. Consequently, the spine will not lengthen as it should on exhalation, and labored breathing results.
See Section 4 Supplement Image 36 for more about ‘Up and over”

Image 4.38 : Neck Muscles
A reminder of the many muscles found in the neck region.
See Section 4 Supplement, Image 37, “Neck Muscles”

Image 4.39 : Dynamic Neutral
We need dynamic neutral to support the arms in free breathing. This dynamic neutral can be interrupted when the collarbone/shoulder blade unit is either back of neutral or forward of neutral (no “shoulders back,” or pulled down). Flute players and string players, especially, may need a reminder of humeroscapular rhythm. Free breath permits free movement of the arm structure for all musicians. Many people intentionally limit the movement of the upper arms in breathing, however the arm structure should be gently responsive to the movement of the ribs underneath.

Image 4.40 : Places of Balance
A reminder, once again, of overall whole body balance and integrating the arms and legs with the movement of breathing.
Questions
-
How has your awareness of your breathing changed from studying this information?
-
How has this work improved your functional efficiency?
Mismappings of Breathing
Some major mismappings of breathing you are likely to encounter when teaching. This doesn’t mean you need to tell everyone. You need to look for these and ask questions to facilitate the clarification (this list is intended to help your eyes see what people are doing).
1. Location and movement of diaphragm
2. Where the air goes
3. Mapping the belly as initiating breathing
4. Size and structure of tongue
5. Location of TMJs
6. Location of trachea
7. Bottom to top event - filling fantasy
8. Arms and legs have nothing to do with breathing
9. Rib cage instead of individual ribs
10. Column - the fantasy of the column of air
11. Lungs push the ribs open
12. Tucking the pelvis, or tightening the glutes provides good support for the breath
© Association for Body Mapping Education August 2023